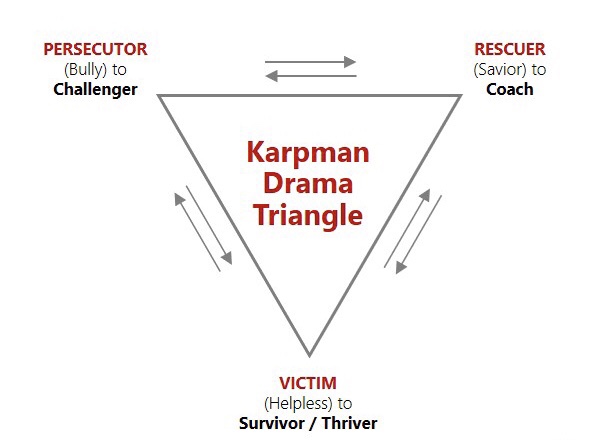
The magical tool to figure this pattern out is called the Drama Triangle. Stephen Karpman created the model in 1968 within the framework of Transactional Analysis. Thanks to this tool we can analyze clearly what is happening in the relationships since the Drama Triangle sheds light on the automatic and dysfunctional interaction between 2 (or more) people.
In a relationship within the Drama Triangle, there are 2 main characters (male or female) who shift from one role to another:
- The Rescuer
- The Persecutor
- The Victim.
The Three Roles In The Drama Triangle
What do the roles entail?
The Rescuer
Rescuers get involved in other people’s lives eagerly waiting for recognition and approval. By making assumptions on other people’s needs they are stepping in to help before anyone has asked them for anything and create a debt of gratitude. They believe that others need them and they impose their solution. In doing so they prevent others from solving their problems themselves. At the same time they manifest their moral superiority.
Feeling responsible for others
Since Rescuers feel responsible for the happiness and well-being of others, they immediately strive to comfort, pacify or calm people down so that these people don’t get to feel their disagreeable emotions like pain, anger, disappointment or sadness. Rescuers also want to have good relationships with everyone, as they like harmony. That is why they avoid conflicts or standing their ground at all costs, even if they end up wasting their time, money or energy. They have a tendency to please people in order to avoid criticism and rejection. After all, they aspire to feel accepted and loved by everyone.
Emotionally disconnected
For all these reasons they are disconnected from their own emotions. Therefore, it is difficult, if not impossible, to have emotional intimacy in a relationship with them. They will flee in “doing”, they are busy at all times … the evidence is their diary: they don’t have a minute.
Codependent relationships
Despite having good intentions, they need Victims to be Rescuers. As a result their behavior encourages the Victim’s dependence and lack of autonomy. Rescuers will continue to be involved in codependent relationships (as with addicts, for example) that are harming them because they do not realize how damaging they are for them.
Saying no is difficult
Rescuers have an imperative need to feel useful to cover up their anxiety and low self-esteem … in short, to give their life meaning. They never stop giving; basically because they don’t know how to say no. However, if they dare to say no, they will feel guilty and label themselves as selfish or stingy. They prioritize others’ needs ignoring their own, because they project on others their own unmet needs. Most of all they have difficulties in identifying their needs and desires.
Am I just nice or too nice?
In short, they sacrifice themselves because they want to prove that they are good, generous and selfless people, who deserve love and recognition. And when someone tells them: “You are too nice”, they feel accordingly offended.
But Rescuing creates resentment and anger in themselves and in the Victims, not recognition, nor gratitude or respect. Whereupon Rescuers confirm their belief that Victims are ungrateful and take advantage of them.
Benefice of the coaching sessions for the Rescuer
When Rescuers attend coaching sessions, working on boundaries and the Drama Triangle guarantees favorable results. Once they have understood the detrimental dynamics and know what their needs are, they are able to control their eagerness to rescue and consequently to change their behavior.
The Persecutor
Am I right or … am I totally right?
Persecutors know everything and are always right. Those who are wrong are the others. Therefore they pretend to know what is best for other people. They characteristically see everything either in black or in white; Grey does not exist. Their motto is: either you are with me or you are against me.
Like Rescuers, they feel morally superior and need Victims in order to play their role as a Persecutor.
Discounting others
They ignore not only other people’s feelings but also their value. That is why they criticize, find fault, persecute, blackmail and abuse their power. In particular they use shame and guilt to manipulate. They can even punish (if only with their moodiness or their silence) so that Victims feel anxious and inferior. Persecutors always find a culprit or an enemy: the other. Thus there is no way to resolve a conflict with them since in each conversation you have to tread carefully and not contradict them. They use threats to get what they want because they have a sense of entitlement. And what they want is for others not only to learn their lesson and to agree with them, but also to change and do things the Persecutor’s way.
Relationships based on power and control
Persecutors feel a lot of anger and righteous indignation, which they vent on “innocent” Victims with gusto. They do not consider themselves as abusive or aggressive though because they believe that the Victims deserve their lot.
In order to feel safe Persecutors want to be in control and they fight for the power in the relationship. They impose their point of view to establish a Winner-Loser relationship that allows them to cover up their inferiority complexes, their insecurity and their vulnerability that they don’t recognize. Moreover they confuse having needs with being needy. Consequently they won’t accept any help or will refuse even to consider that someone can do something for them.
Others are to blame
But there will always be somebody to blame, somebody who doesn’t meet their expectations. When something goes wrong, Persecutors hold others accountable for what happens to avoid blaming themselves. With that attitude it seems unlikely that they will attend coaching sessions since the person responsible or the culprit is always the other. They project on others (outside of themselves) what they don’t want to see in themselves. In effect, they would call others arrogant because they are not able to recognize and accept their own arrogance.
Childhood trauma
As they have often suffered some kind of abuse in childhood, they always get defensive. They reproduce the behavior of the abuser because they hope that by dominating others they will preventively protect themselves from abuse or contempt.
The Victim
Discounting themselves
Victims feel powerless, incompetent, stuck and sometimes desperate. They discount their skills and their resources. They don’t recognize their own ability to change things or to influence their destiny either. Besides, precisely because life happens to them, they often suffer from depression. And if by miracle something good happens, they attribute it to luck.
Not owning it
According to Victims they can’t be blamed for anything because they are not responsible. What’s happening is not their fault. They are convinced that life is very hard, that nobody understands them and that no matter what they do they will be unable to change their lot. They always find excuses that justify their situation.
Avoiding responsibilities
Victims take any opportunity to complain; even their usual tone of voice is querulous. They are the eternal victims of life itself and manage to get sick, have ailments and attract misfortunes. As soon as they get stressed, which happens very easily, they make a mountain out of a molehill. They simply avoid responsibilities and don’t want to make decisions for fear of being wrong.
In addition, you can recognize Victims by their usual way of apologizing for everything and nothing. You can often hear them say “Sorry!”, “Excuse me!”, “I beg your pardon!”.
“A Victim is someone who is waiting for something bad to happen … and it usually does.”
~ Barry K. Weinhold
Not only do they live in an illusory world composed of all the things they imagine or assume (dire consequences, negative emotions or adverse reactions of others, …), they also make assumptions without relying on reality, without having sound evidence that would justify their beliefs.
Passivity
Of course Victims adopt a passive behavior: they don’t take action, they don’t make any effort to get out of the pothole. They are experts in manipulating others to get what they need without getting too involved in the result. They usually sabotage the help they receive and secretly rejoice in their failures. No matter how often they attend coaching sessions, their passivity and lack of commitment may cause the attempt to fail, so that they can blame the coach for the lack of results and prove them incompetent.
Two types of Victims
Victims attract either Rescuers or Persecutors. On the one hand, Victims create codependence – an excessive emotional or psychological dependence on the Rescuer. This attitude encourages a passive behavior that prevents them from developing fully their abilities. On the other hand, Victims confirm their belief that life is hard and unfair when they are abused by Persecutors.
Therefore, to play their role as Victims they need Rescuers or Persecutors … or both.